
1Institute for Work & Health, 2University of Toronto, 3Toronto Western Hospital - University Health Network, Toronto, Canada, 4Russian National Resarch Medical University, Moscow, Russia, 5Christian Medical College, Vellore, India, 6Toronto Rehabilitation Institute- University Health Network, Toronto, Canada and 7University of Antioquia, Medellin, Colombia
Objective: To compare models of rehabilitation services for people with mental and/or physical disability in order to determine optimal models for
therapy and interventions in low- to middle-income countries.
Data sources: CINAHL, EMBASE, MEDLINE, CENTRAL, PsycINFO, Business Source Premier, HINARI, CEBHA and PubMed.
Study selection: Systematic reviews, randomized control trials and observational studies comparing >2 models of rehabilitation care in any language.
Date extraction: Standardized forms were used. Methodological quality was assessed using AMSTAR and quality of evidence was assessed using GRADE.
Data synthesis: Twenty-four systematic reviews which included 578 studies and 202,307 participants were selected. In addition, four primary studies were included to complement the gaps in the systematic reviews. The studies were all done at various countries. Moderate- to high-quality evidence supports the following models of rehabilitation services: psychological intervention in primary care settings for people with major depression, admission into an inpatient, multidisciplinary, specialized rehabilitation unit for those with recent onset of a severe disabling condition; outpatient rehabilitation with multidisciplinary care in the community, hospital or home is recommended for less severe conditions; However, a model of rehabilitation service that includes early discharge is not recommended for elderly patients with severe stroke, chronic obstructive pulmonary disease, hip fracture and total joints.
Conclusion: Models of rehabilitation care in inpatient, multidisciplinary and specialized rehabilitation units are recommended for the treatment of severe conditions with recent onset, as they reduce mortality and the need for institutionalized care, especially among elderly patients, stroke patients, or those with chronic back pain. Results are expected to be generalizable for brain/spinal cord injury and complex fractures.
Key words: disabled persons; rehabilitation; rehabilitation centres; activities of daily living; delivery of healthcare; mortality; quality of life; disability.
Accepted Jan 17, 2018; Epub ahead of print Apr 3, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Andrea D. Furlan, Division of Physical Medicine and Rehabilitation, Institute for Work & Health, 481 University Av, Suite 800, Toronto, ON M5G 2E9, Canada. E-mail: afurlan@iwh.on.ca
We reviewed the published scientific literature to identify the best rehabilitation models for the World Health Organization guideline of Rehabilitation in Health Systems, which was released in 2017. Rehabilitation can be delivered in various different settings, for people with major depression it is better to receive psychological interventions in primary care; for people with a severe disabling condition, it is better to be admitted to an inpatient, multidisciplinary or specialized rehabilitation unit; for people with less disabling conditions, they can receive rehabilitation in outpatient settings with a multidisciplinare team. Elderly people with severe stroke and other diseases should not be discharged early from hospital. These results are especially important for low- and middle-income countries to know which rehabilitation model is better so they can invest their human and financial resources appropriately.
Strong evidence is needed to inform the development and implementation of rehabilitation services worldwide. According to the World Report on Disability produced by the World Health Organization (WHO) and the World Bank, there are more than 1 billion people with disabilities in the world, of which approximately 80% live in low- and middle-income countries (LMIC) (1). The WHO Disability Action Plan 2014–2021 emphasizes the need for guidance to develop and strengthen rehabilitation services. It prioritizes: removing barriers and improving access to health services and programmes; strengthening and extending rehabilitation, habilitation, assistive technology, assistance and support services; and strengthening the collection of relevant and internationally-comparable data on disability and related services (2).
Evidence-informed programmatic guidelines play a critical role in strengthening rehabilitation services and outcomes, as they provide guidance to ensure that programmes and services are appropriately timed and targeted to support optimal health, quality of life (QoL) and functional ability. This is of particular relevance in LMIC, where infrastructure, access to trained personnel, and finance is often limited and must be efficiently utilized. It is even more important to improve availability, accessibility and affordability of rehabilitation services in order to overcome barriers to referral, such as inaccessible locations, inadequate services, and the high costs of private rehabilitation (1). Many barriers to implementation of the WHO Disability Action Plan 2014–2021 have been identified by LMIC; for example, engagement of health professionals and institutions using a multi-sectorial approach, new partnerships, strategic collaboration, provision of technical assistance, future policy directions, and research and development (3).
A variety of rehabilitation service models exist for those with physical and/or mental disabilities; however, it is unknown which models of care are optimal for specific populations, settings and conditions. Although it would be desirable to evaluate the intrinsic components of each rehabilitation service model (e.g. care plans and presence of gatekeeping function), it would be a monumental task to assess these components individually, and therefore we opted to study rehabilitation service models from a wider perspective.
This systematic review was conducted in response to a call by the WHO to provide best available evidence to support the development of new WHO guidelines on health-related rehabilitation models and services for people with physical and/or mental disabilities. Rehabilitation models and services include the place where rehabilitation is delivered (community-, hospital-, clinic or facility-based rehabilitation), the distribution system (integrated, decentralized or centralized services), the professional interactions (multidisciplinary or non-multidisciplinary), the levels of expertise offered (specialized units or general wards), and leadership and governance (integrated into health services or into social and welfare services).
This review describes best available evidence on rehabilitation service models and their optimal use for the treatment of physical/mental disability in LMIC. Evidence was used to inform the development of the 2017 WHO guidelines: Rehabilitation in Health Systems (4).
This systematic review was designed using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist (5). The review protocol, including eligibility criteria, is available on request from the authors.
Nine electronic databases were searched: CINAHL, EMBASE, MEDLINE, CENTRAL, PsycINFO, Business Source Premier, HINARI, CEBHA, and PubMed. Hand searching was used to capture grey literature and relevant reports. All literature published during 1994–2014 that met the inclusion criteria was included.
The search strategy for this review is shown in Appendix SI1. Key terms were identified to populate the PICO categories (Population, Intervention, Comparison and Outcomes) and were combined as follows: all terms within a category were combined using a Boolean “OR” operator. The 4 categories were then combined with a Boolean “AND” operator, ensuring that captured articles contained at least 1 term from each of the categories. Searches were not limited by study design. All searches were conducted by an experienced librarian with input from the research team.
Complementary searches to find primary studies (randomized controlled trials (RCTs) or observational studies) were conducted in PubMed. A focused website review was conducted to ensure the inclusion of relevant reports. Additional searches were conducted in key websites, such as the Spinal Cord Injury Rehabilitation Evidence (SCIRE) website (6). Any additional articles of relevance were screened along with the other sources of literature. Grey literature and online resources are shown in Appendix SI1.
Search results were downloaded into Reference Manager® (7) to remove duplicates, and were then uploaded to DistillerSR® (8), a web-based systematic review software designed for screening and data extraction phases. Inclusion and exclusion criteria were developed and pilot tested by the research team before screening began. Pilot results were compared and conflicting responses discussed until everyone was comfortable with the inclusion/exclusion criteria.
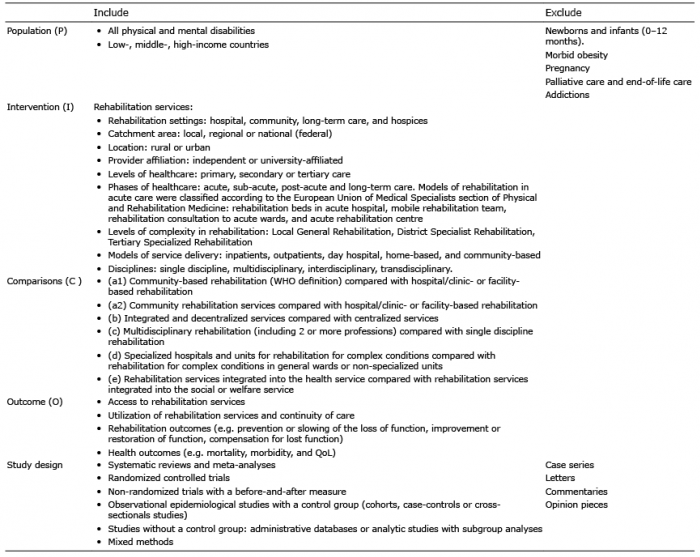
Systematic reviews, meta-analyses, RCTs, and non-randomized studies comparing 2 or more service delivery models meeting the PICO criteria were included, as shown in Table I.
Table I. Inclusion and exclusion criteria
Standardized data extraction forms were developed in conjunction with WHO staff, and pilot-tested by the team, who met regularly.
Two independent reviewers conducted quality appraisal and data extraction using standardized data extraction forms. Reviewers compared appraisal forms, discussed discrepancies, and achieved consensus. The following items were extracted: authors, country, year, LMIC yes/no, population, models of care, outcomes and results, as well as information required for assessing quality of the study. RCTs and observational studies were assessed for the following risk of biases: selection, performance, measurement and attrition.
All systematic reviews were assessed using the AMSTAR criteria (9) to judge their methodological quality. When a systematic review did not conduct or report adequate critical appraisal of the included articles, researchers conducted an independent assessment using the Cochrane Collaboration Risk of Bias tool for selection, performance, measurement, attrition, and reporting biases.
Quality of evidence was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) tool (10). Pre-specified criteria were used to judge the quality of the evidence, including study design, study limitations, inconsistency, indirectness, imprecision, and publication bias. The GRADE assessment reviewer guide is shown in Appendix SI1. Given that this review was conducted to support rehabilitation guidelines for LMIC, outcomes that included studies conducted in high-income countries were downgraded due to indirectness. The quality of evidence for each comparison was categorized as follows:
The evidence available to answer each sub-question began the grading process with a “High” grade when the evidence was based on RCTs, and “Low” grade when the evidence started with observational studies. GRADE tables are shown in Appendix SII1.
A total of 8,990 publications were screened and 740 articles were retrieved for full-text review. Of these, 24 systematic reviews and 4 primary studies were included. Fig. 1 shows the flow of articles according to the PRISMA guideline. The most common reason for exclusion was that 2 models of rehabilitation services of interest were not compared. Included and excluded studies are listed in Appendix SI1.
Fig. 1. Flowchart of studies for Population, Intervention, Comparison and Outcomes (PICO) question. RCT: randomized controlled trial.
Table II presents the characteristics of each systematic review and primary study including their individual AMSTAR appraisal outcomes. Table III shows extracted data and results for each PICO question. Individual GRADE tables are shown in Appendix SII1.
A1. Hospital at home: Early discharge from hospital with rehabilitation at home. There is “moderate quality” evidence that providing services at home after being discharged early is associated with an increased risk of re-admission for people with severe stroke, chronic obstructive pulmonary disease, hip fracture and total joints (11). Subgroup analyses demonstrated a significant interaction (p = 0.04) for stroke severity: there was a reduced likelihood of death or dependency in people with moderate stroke severity (initial Barthel Index > 9), but not in the severe subgroup (initial Barthel Index 0–9). There was also a significant interaction (p = 0.0002) for the reduction in duration of hospital stay, which was much greater for the severe stroke subgroup (38). There is “low-quality” evidence that providing services to people at home after being discharged early is not associated with increased risk of death or re-admission in the subgroup of people with stroke, and older people with chronic obstructive pulmonary disease (COPD) (11). There is “low-quality” evidence that providing services to people at home after being discharged early is not associated with poor function, such as dressing or activities of daily living for older people with a mix of health conditions (11). There is “low-quality” evidence that providing services to people at home after being discharged early is not associated with increased mortality in people with mixed conditions, and in those with COPD (11).
There is “moderate-quality” evidence that integrated rehabilitation is better than usual care for patients with COPD, measured according to hospital admissions. There is “low-quality” that integrated rehabilitation is better than usual care for the rehabilitation outcome of 6-Minute Walk Distance (6MWD). There is “moderate-quality” evidence that integrated rehabilitation is better than usual care for QoL. There is “very-low-quality” evidence that integrated rehabilitation is no different from usual care for mortality (24). There is “very-low-quality” evidence that living in a community with an Integrated Service Delivery (ISD) network is better than living in a community without one, for elderly people (> 75 years old) with moderate level of disability and mild cognitive problems, with outcomes of utilization of rehabilitation services and continuity of care. An ISD network reduces the number of elderly people with unmet needs and also reduces the prevalence of unmet needs (25). There is “very-low-quality” evidence that new models of “cooperative care” that link primary care providers and local services with regionalized adult-centred specialty services may make it possible to offer a meaningful transition experience to young people with chronic conditions. The authors identified 5 key elements that support a positive transition to adult-centred healthcare: preparation, flexible timing, care coordination, transition clinic visits, and interested adult-centred healthcare providers. Overall, there is limited empirical evidence related to the process and outcomes of the transition to adult-centred healthcare for people with cerebral palsy and spina bifida (26). There is “very-low-quality” evidence that there is no difference between individualized care coordination and standard care delivered by paediatrician’s offices for families with complex healthcare needs in terms of reducing unmet needs (27). However, there is “very-low-quality” evidence that the care coordination model is better than standard care for utilization of rehabilitation services assessed with the use of specialist care (27).
There is “very-low-quality” evidence that multidisciplinary rehabilitation involving a graded 4-part activity programme is better than traditional care for disability and for return-to-work for people with sub-acute low-back pain (34).
There is “very-low-quality” evidence that multidisciplinary biopsychosocial rehabilitation (psychological coaching setting) is no better than a biopsychosocial rehabilitation with psychologist contact only for disability for people with neck and shoulder pain (32). There is “very-low-quality” evidence that active multidisciplinary rehabilitation is no better than traditional rehabilitation for sick leave (33).
This comparison was not made, as no systematic reviews or primary studies were found.
This review provides evidence to support a variety of service delivery models for complex cases of disability. Stroke is one of the most complex conditions for rehabilitation because it can affect motor, sensory, cognitive, affective, and coordination systems. Moreover, rehabilitation of elderly patients is one of the most challenging situations, given that co-morbidities are more frequent in this age group, and their home environment may not be conducive for discharge after rehabilitation. Evidence was found on rehabilitation services for many other conditions causing physical and/or mental disability, such as those affecting cardiac (CHF), pulmonary (COPD, asthma), neurological (brain injury, spinal cord injury, ALS, MND) and musculoskeletal systems (hip fractures, low-back pain, neck pain, shoulder pain), as well as those for paediatric populations (cerebral palsy, spina bifida), and populations with cancer and mental health conditions (intellectual disability, depression, schizophrenia).
This review highlights a need for high-quality research in a number of areas. First, there is an urgent need for more research conducted within LMIC. This is extremely important to assist in judgements of feasibility and resource needs for the implementation of recommendations in resource-limited settings. Specifically, there is a need for RCTs and systematic reviews assessing different models of rehabilitation care in a variety of care settings. For example: community rehabilitation services offered at home compared with services offered at the general practitioner’s office. Future research should also focus on measuring outcomes of access to rehabilitation, utilization of services, continuity of care, functional ability and QoL.
Secondly, many conditions have been poorly studied regarding rehabilitation models. These conditions are: spinal cord injury, amputees, paediatrics, cancer and acquired brain injury. There were no studies comparing service models for populations with amputations. However, various authors, drawing from experiences with the Veteran Affairs and Departments of Defense, suggest that the rehabilitation of a person with an amputation should be carried out by a multidisciplinary rehabilitation team in a specialized centre (39–41).
Thirdly, as part of our PICO question, we searched for literature on rehabilitation services integrated into health services compared with rehabilitation services integrated into social and welfare services; however, no relevant literature was found on this topic because no comparative studies exist in this area. At the time of this review, another team prepared a realist synthesis for the WHO rehabilitation guideline on the topic of leadership and governance of health-related rehabilitation (42). One principle that emerged from their research findings was to “institutionalize” rehabilitation programmes by aligning programmes with well-known, pre-existing Ministerial models of healthcare, similar to other Ministerial programmes, in order to support programme sustainability. It is also recognized that governance, political will and a common understanding of disability and rehabilitation are crucial for implementation of the recommendations in the rehabilitation guideline (43).
Finally, of the outcomes extracted, very few studies measured whether a specific service model improved access to rehabilitation services. There were many gaps in the provision of, and access to, rehabilitation services, and this is important for people with disabilities, given the many barriers to accessing healthcare. No high-quality direct evidence was found that some service delivery models increase access to rehabilitation services. There is a need for more research in this area, especially for studies that compare community-based services with specialized centres, where access to rehabilitation services may require travel, transportation and lead to caregiver burden.
This review paper relies primarily on evidence from systematic reviews published in the last 20 years. In cases where no systematic review was found, primary studies (trials and observational studies) retrieved by our main search strategies were included. Despite the range of strategies to find studies, no evidence was found of rehabilitation models for a variety of disabling conditions, such as amputations and cancer, and very few observational studies were found for spinal cord injury, acquired brain injury, and paediatric conditions, such as spina bifida or cerebral palsy. Although our searches were comprehensive, a possible limitation could be the electronic searches used in this review. A further limitation of this review is that most of the evidence came from high-income countries, and therefore the application to LMIC needs to be assessed. Lastly, the recommendations are based on RCTs, many of which had a lack of blinding. This was expected given the nature of these interventions, but the lack of blinding introduces a risk of performance and measurement biases. Measurement bias is less likely for objective measures, such as mortality and hospital re-admissions; however, such bias can be reduced by blinding outcome assessors on other rehabilitation outcome measures. Many studies also had high risk of selection, attrition and reporting biases. In a few instances, it was possible to assess for publication bias, and there was no indication that this was a problem in this review.
There is moderate-to-high-quality evidence to support that those experiencing the recent onset of a severe condition (with the potential for major and complex disability) should be admitted to an inpatient, multidisciplinary, specialized rehabilitation unit, and continue rehabilitation as an outpatient until the rehabilitation goals are achieved. This approach will reduce mortality and the number of people admitted into institutional care. The evidence is stronger for elderly patients, stroke patients, and those with chronic low-back pain, but it is expected these outcomes are generalizable for people with brain injury, spinal cord injury, and complex fractures (e.g. fragility fractures in older adults). There is moderate-quality evidence that people with less severe or complex conditions should be rehabilitated in outpatient settings with a multidisciplinary team (including 2 or more professions), either in a community service or clinic-, hospital-based service (day hospital) or in-home (domiciliary) rehabilitation. For those with mental health conditions, multidisciplinary care, including psychological interventions and intensive case management, is recommended. Early discharge from hospital with rehabilitation at home is not recommended for elderly patients or those with mixed conditions, as evidence suggests it is more harmful than beneficial.
The authors would like to thank Dr Marta Imamura, Ms Joanna Liu, Ms Manisha Sachdeva, Dr Fernando Quadras Ribeiro, Ms Mary Cicinelli and Ms Jocelyn Dollack for their assistance during the review process.
Funding: The team received financial support from Lucy Montoro Rehabilitation Network - University of Sao Paulo Medical School – Brazil on behalf of the World Health Organization for the conduct of this review. The WHO provided clarification and methodological guidance throughout the process.
Excluded studies: Available on request.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize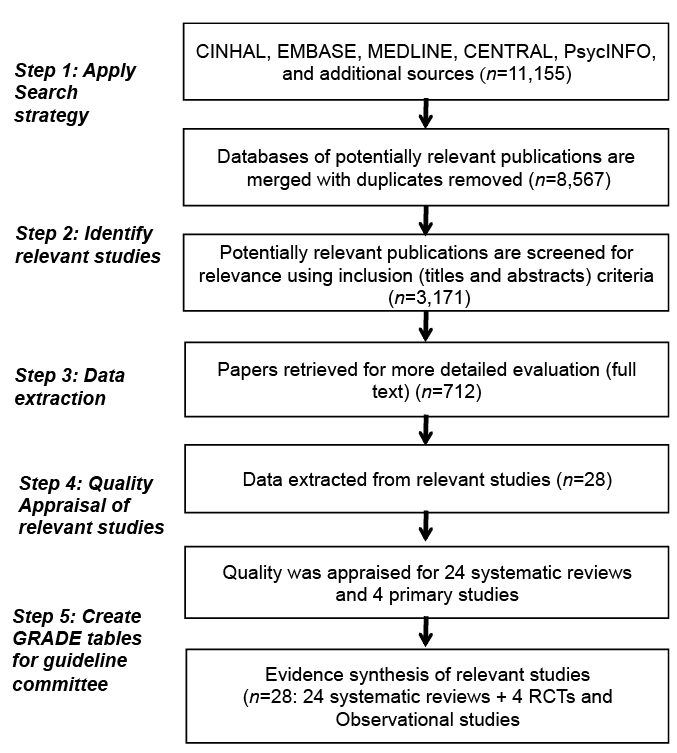 Click to show fullsize
Click to show fullsize
